

Disposable America: Growing Old Without Dignity
The collapse of elder care is making aging a slow erasure.

Note: This article is part 3 in our Disposable America series regarding healthcare.
Aging in a country that worships youth and profit is a recipe for erasure. Today’s aging population knows this firsthand. And if something doesn’t fundamentally change, so will many generations to come.
In America, growing old is a liability, not a legacy, not a season of rest, just a cost to be managed. We celebrate longevity in theory, but in practice, we abandon it.
This country has spent decades dismantling the systems that once helped people age with dignity. Families are scattered, safety nets are shredded, and elder care has been handed over to the private sector to be monetized, minimized, or denied altogether.
The result is a quiet catastrophe: elders dying alone in understaffed facilities, bankrupted by care, or locked into systems that strip away their autonomy in the name of “protection.” Many never had a shot at care to begin with. Others are cared for only as long as the money lasts.
We’ve turned one of life’s most universal stages into a bureaucratic death spiral and then told people it’s their fault for not planning better.
This isn’t about personal failure. It’s about policy. It’s about profit. And it’s about what happens when a nation that worships youth and productivity decides it can no longer afford to let its elders live with dignity.
In this chapter of Disposable America, we examine how our systems—from Medicaid and Medicare to housing, labor, and healthcare—turn aging into a punishment. We follow the money, trace the policy, and listen to the people left behind.

Coffman Chronicles
We just hit 13,000 subscribers—thank you! To celebrate, we’re offering full access to The Coffman Chronicle at 50% off.
Get exclusive analysis and fearless reporting you won’t find in corporate media.
Support truth. Stay informed.
A System Built to Fail: The Fall of Long-Term Care
If a society's test is how it treats its elders, America is failing—and not by accident. The collapse of elder care in this country isn’t a tragedy; it’s a strategy.
The federal government began retreating from elder care decades ago. Public investment dried up in the post-Reagan era, leaving long-term care to be filled by for-profit chains and underfunded state programs. The result? A fragmented, deeply unequal system where quality depends on your zip code and your income.
COVID pulled back the curtain. Tens of thousands of nursing home residents died not just from the virus, but from years of understaffing, disrepair, and regulatory failure. But the crisis didn’t start in 2020. That was just the moment the rest of the country noticed.
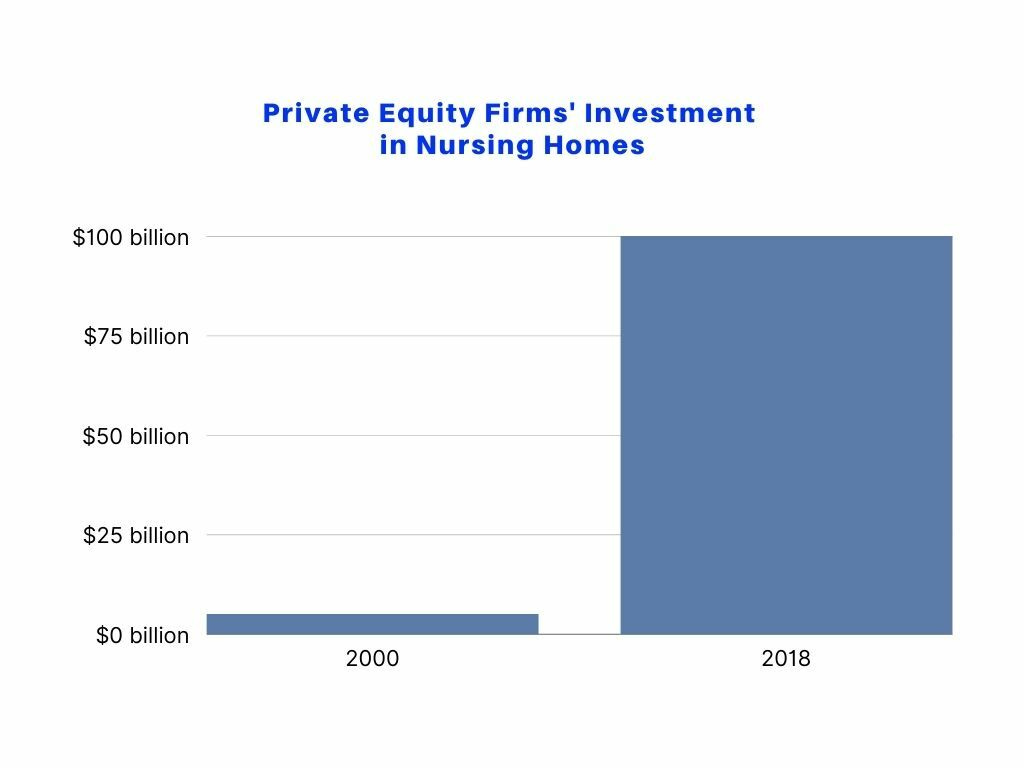
Today, many of the country’s largest elder care providers are owned by private equity firms. Their business model is simple: cut staff, cut training, cut costs, and extract as much profit as possible before flipping the property or dissolving the LLC.
Regulators, meanwhile, are either toothless or captured. In many states, the agencies tasked with oversight are the same ones slashing funding for home-based alternatives. As a result, even “good” facilities struggle to maintain quality, while the worst operate with impunity.
While the institutional model limps along, the promise of home-based care remains mostly that—a promise. Waiver programs have waitlists that stretch into years. Caregiver wages are stagnant. Infrastructure for aging in place is either unfunded or nonexistent.
Long-term care isn’t broken. It’s functioning exactly as designed—for those who profit from other people’s decline.
From Interdependence to Isolation
Aging used to mean staying close to home. For generations, elder care was rooted in family, community, and shared responsibility. Parents lived with their adult children, and grandparents helped raise grandchildren. In many Indigenous, immigrant, and working-class households, this interdependence wasn’t a backup plan—it was the plan.
But American capitalism had other ideas.
As work became more mobile, housing became more expensive, and caregiving became more invisible, the structures that supported multigenerational living were systematically undermined. Job markets and redlining pushed families apart. Wages stagnated while caregiving responsibilities multiplied. Aging in place became an aspiration only the wealthy could afford.
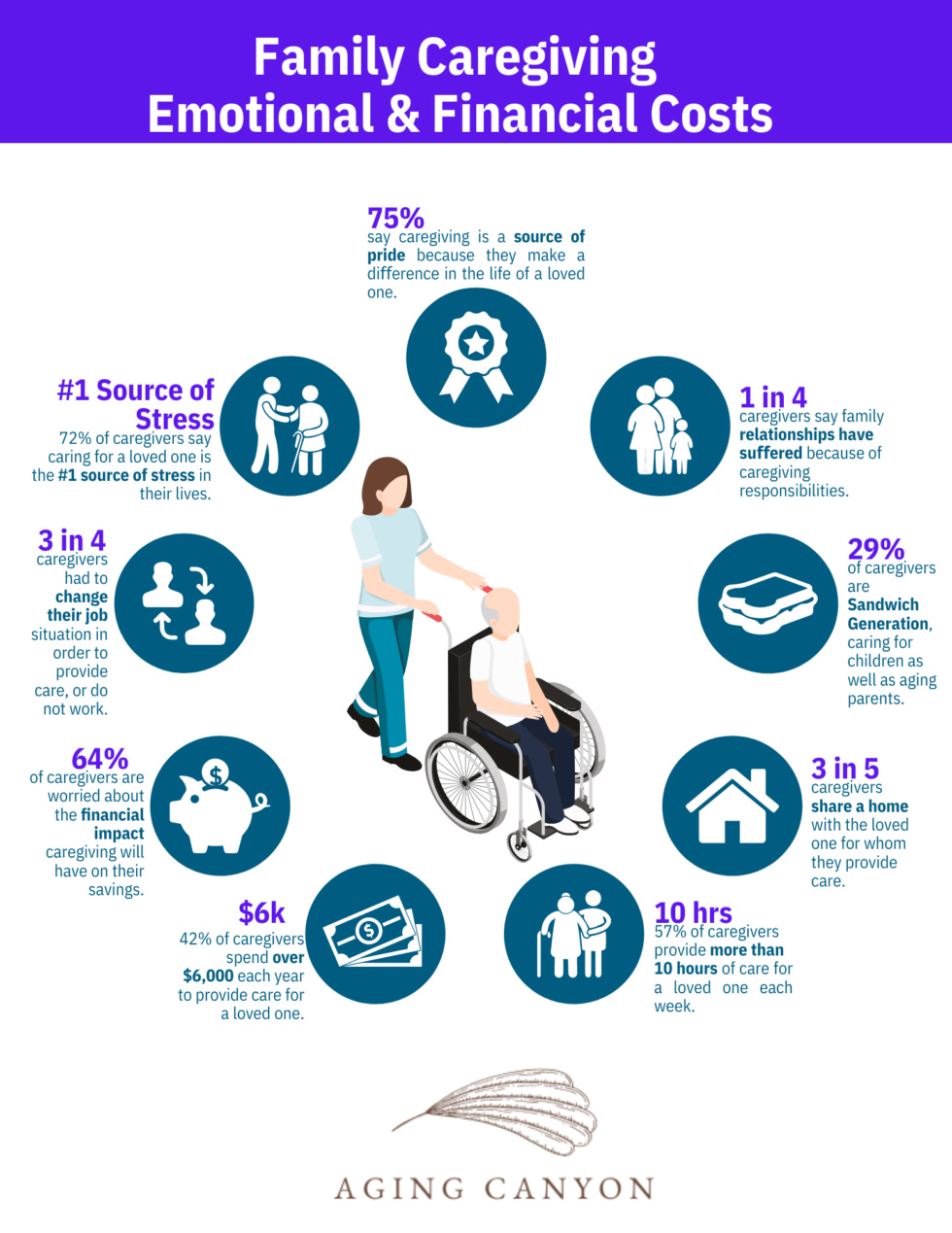
Even when families do try to step in, the cost is enormous—financially, emotionally, and physically. For every grandparent who "ages in place," there’s a working child or grandchild quietly burning through their PTO, sacrificing income, or pulling double duty after a shift. And when wages are low, paid leave is nonexistent, and home care is inconsistent at best, the cracks widen fast.
In-home care, when it’s available, often covers only an hour or two a day—barely enough for basic hygiene, let alone companionship or oversight. On weekends, support disappears. Waitlists stretch for months. One missed window, one hospitalization, and you’re back to zero. The system resets, but your parent doesn’t.
In many families, the stress isn’t just unsustainable; it’s unsafe. Everyone’s health suffers. Everyone’s stability teeters.
This isn’t just an American story. It’s a global one. In Japan, the world’s oldest society by median age, elder abandonment is so common that “lonely death” (kodokushi) has become a sociological category. In China, rapid urbanization has pulled younger generations away from rural villages, leaving aging parents behind with little support. Across Europe, care networks are collapsing under the combined weight of aging populations, austerity politics, and privatized labor markets.
What once bound families together—proximity, tradition, shared survival—has been eroded by market forces and migration. Where once multiple generations shared the same home or street, today’s elders often find themselves alone, aging far from children who now live across states, continents, or class divides. Many continue working well past retirement age, not out of choice, but necessity—until their health gives out and the only available “solution” is institutionalization or isolation.
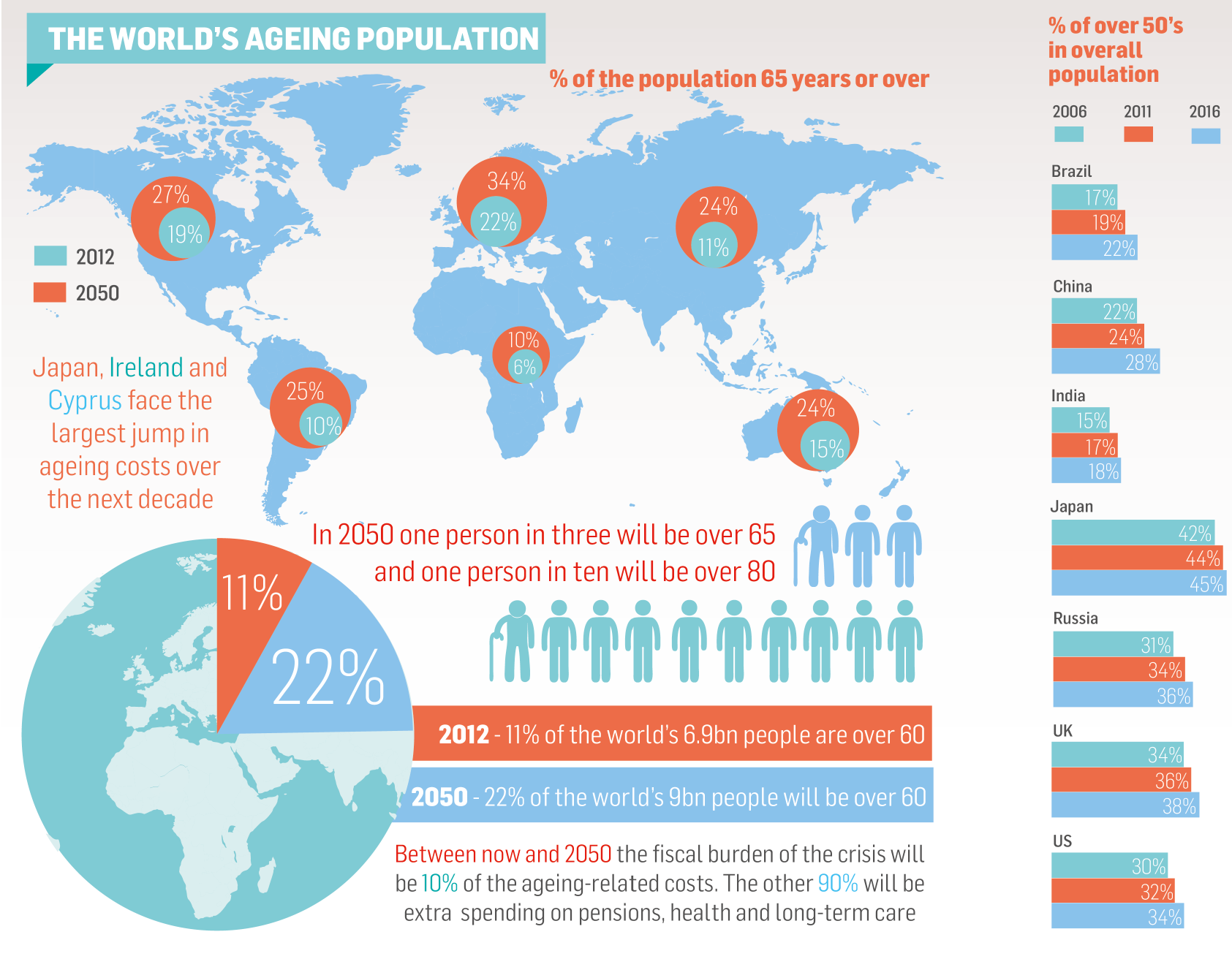
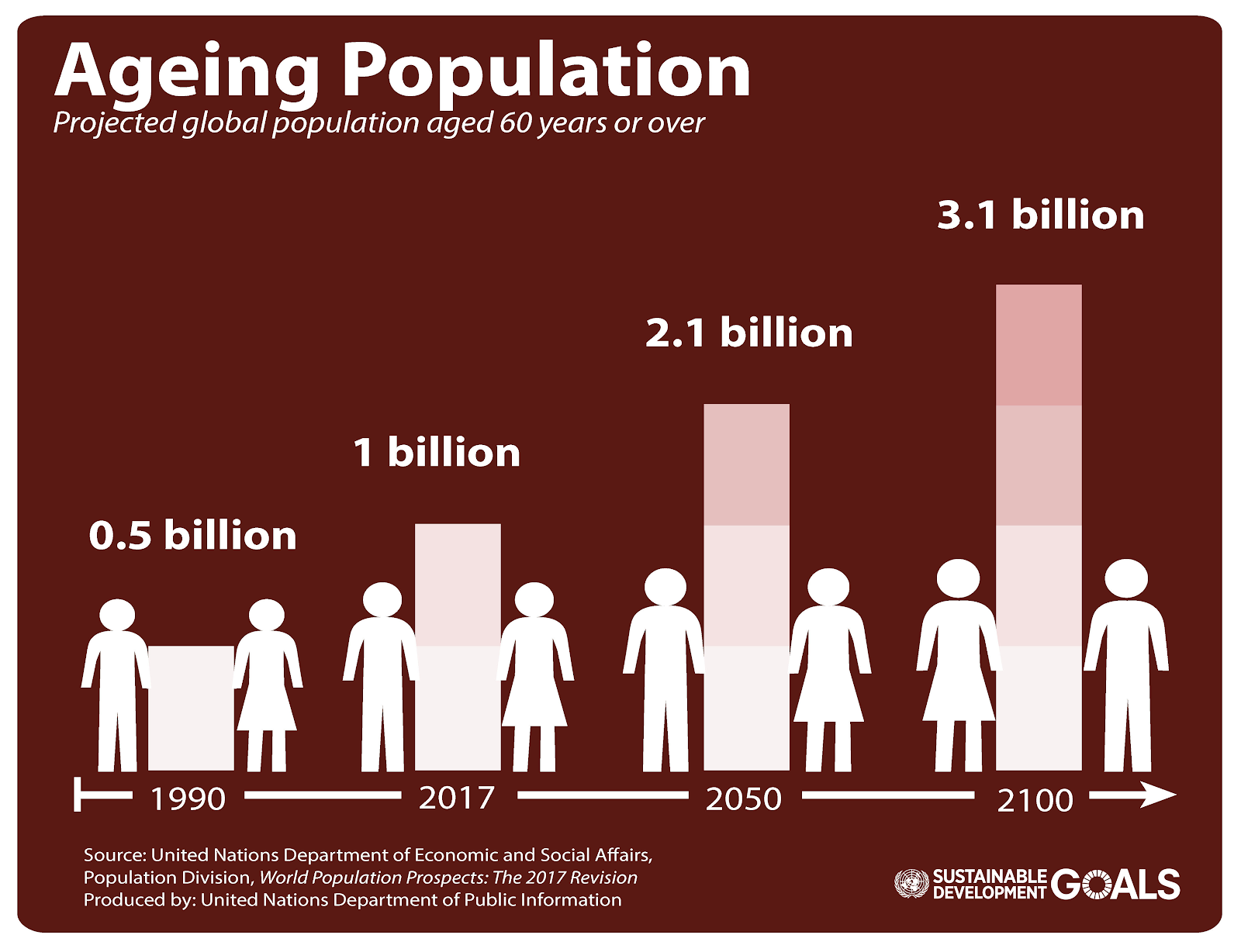
And the numbers are only moving in one direction. By 2034, adults over 65 will outnumber children under 18 in the U.S. for the first time in history. At the same time, birth rates continue to fall, and caregiving labor, already underpaid and overextended, isn’t being replenished.
We are aging into a structurally unequipped society to care for the people who built it. Without massive investment and cultural shift, today’s crisis will become tomorrow’s collapse.
Medicaid Maze, Medicare Gaps, and Wealth Extraction
For many Americans, the first real encounter with the elder care system doesn’t happen until someone they love needs help; by then, it’s too late. What they find isn’t a safety net. It’s a trapdoor.
Medicare doesn’t cover long-term care in this country. It isn’t free. It isn’t even affordable. It’s an asterisk on every health policy brochure: a massive, life-altering need that’s been quietly excluded from the programs most people assume will protect them.
Private insurance won’t save you either. Long-term care policies are expensive, filled with exclusions, and often inaccessible to anyone who actually needs them. And when they do pay out, it’s frequently too little, too late. As of 2024, fewer than 7% of Americans over 50 had any long-term care coverage, and many policies have caps or “use it or lose it” clauses that punish proactive planning.
That leaves Medicaid, the last-resort safety net. But to qualify, most people have to spend down nearly all their assets, including their homes. Families are forced to cash out retirement accounts, sell property, or give up inheritances just to keep a parent in care.
This isn’t just personal financial devastation. It’s intergenerational wealth extraction. Whole families are being drained to keep elders housed and medicated, while nursing home corporations report record profits and states quietly slash home-care budgets.
The result is a system where the poor suffer, the middle class falls, and only the wealthy get options. Everyone else? They get on a waitlist, go bankrupt, or hope they die before the next premium hike.
You may also enjoy our previous reporting in this series. Start here:

Who Gets Left Behind: Race, Class, and Queer Aging
The crisis in elder care doesn’t fall evenly. It falls hardest on those who’ve always been pushed to the margins—Black, Brown, disabled, poor, and queer elders—people who were already navigating injustice long before old age made them “visible.”
In many states, majority-Black or Latinx nursing homes receive significantly less funding and oversight. Staff are underpaid, turnover is constant, and basic care suffers. The racial wealth gap doesn’t disappear in retirement; it widens.
Indigenous elders face another crisis: geographic isolation and systemic neglect. Rural reservations often lack elder housing or healthcare facilities entirely. Tribal-run elder programs are chronically underfunded, and transportation barriers cut off access to even basic care.
For LGBTQ+ elders, the risks are uniquely acute. Many are aging without partners, children, or legal protections. Others fear entering long-term care facilities where they might be forced back into the closet. Discrimination from staff or fellow residents isn’t hypothetical; it’s documented. One 2023 study found that 34% of LGBTQ+ seniors faced some form of abuse or neglect in institutional care.
Disabled elders often face the worst of both worlds. If they’ve been disabled for decades, they may already be stuck in the institutional system. If they’re aging into disability, they’re often forced to “prove” their needs to state bureaucracies trained to deny benefits. Guardianship laws, which can strip people of their rights in the name of safety, disproportionately target those who can’t afford to fight back.
In other words, if you’re aging while marginalized, the system doesn’t forget you. It targets you again.
The For-Profit Elder Economy
In today’s America, growing old is a market opportunity for someone else. Elder care isn’t treated as a right. It’s treated as a revenue stream.
Private equity firms now own the largest nursing home chains in the country. Their goal isn’t to provide care; it’s to extract profit. The playbook is simple: acquire facilities, cut staffing, slash wages, reduce training, and outsource services to shell companies. Then, sell the business or declare bankruptcy, often while continuing to operate under a new name.
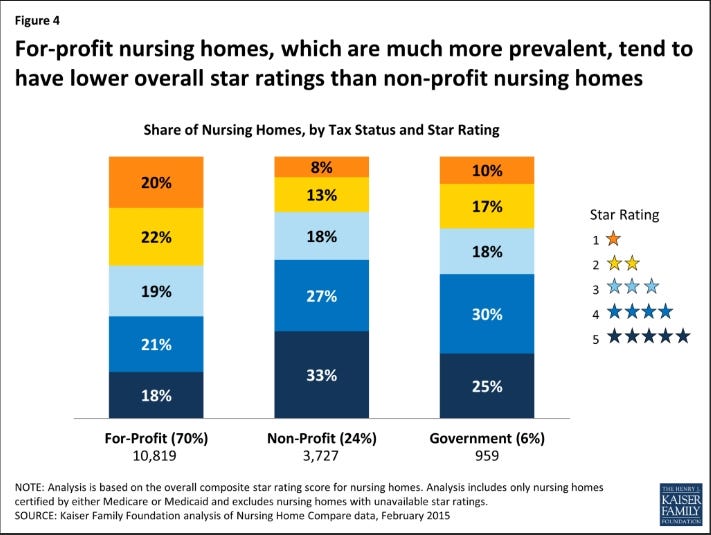
According to the Centers for Medicare & Medicaid Services, residents in private equity-owned facilities are significantly more likely to experience preventable hospitalizations and emergency visits. They’re also more likely to live in homes with fewer nurses, lower inspection scores, and chronic understaffing. But that’s not considered failure. It’s considered efficient.
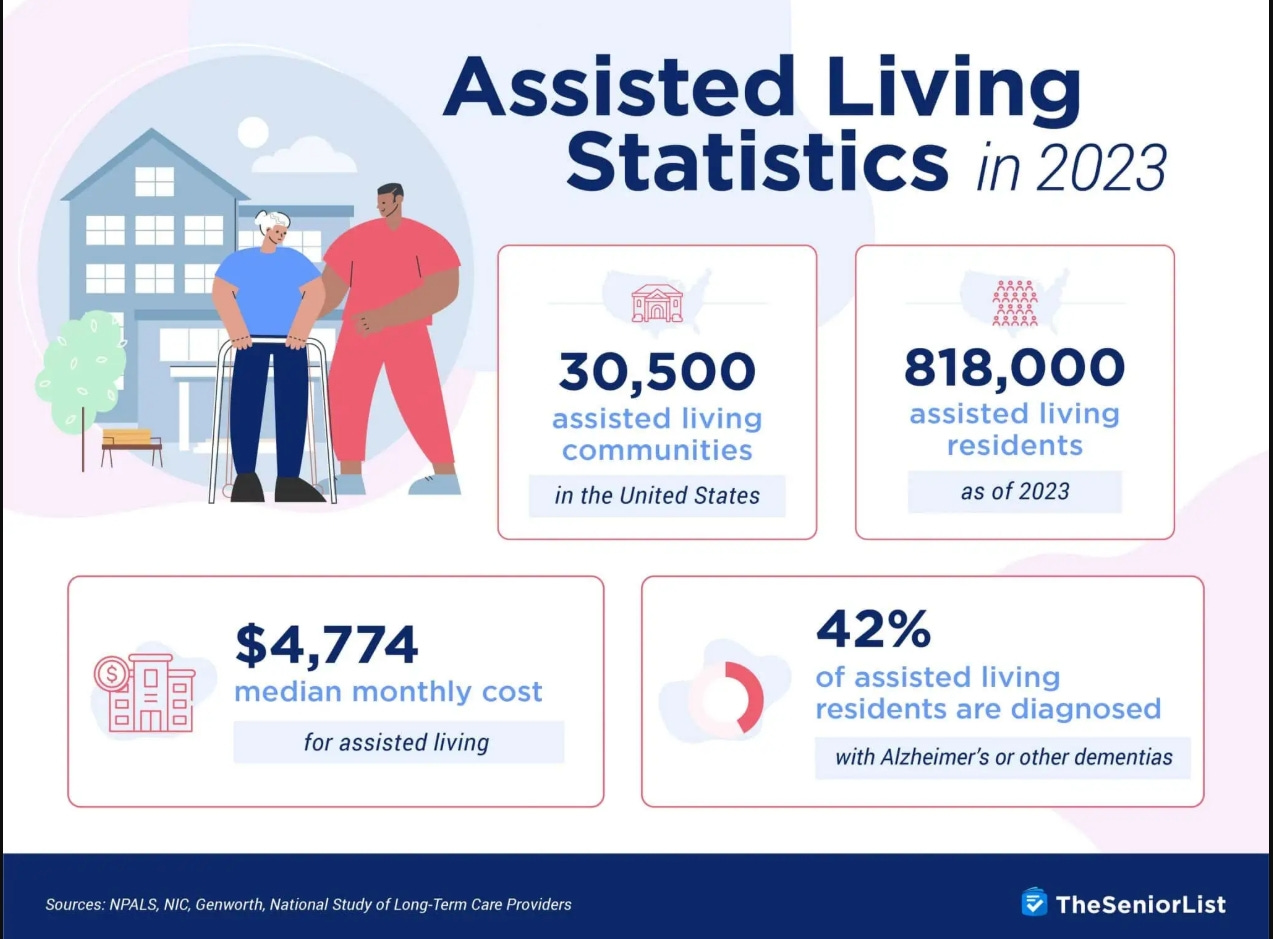
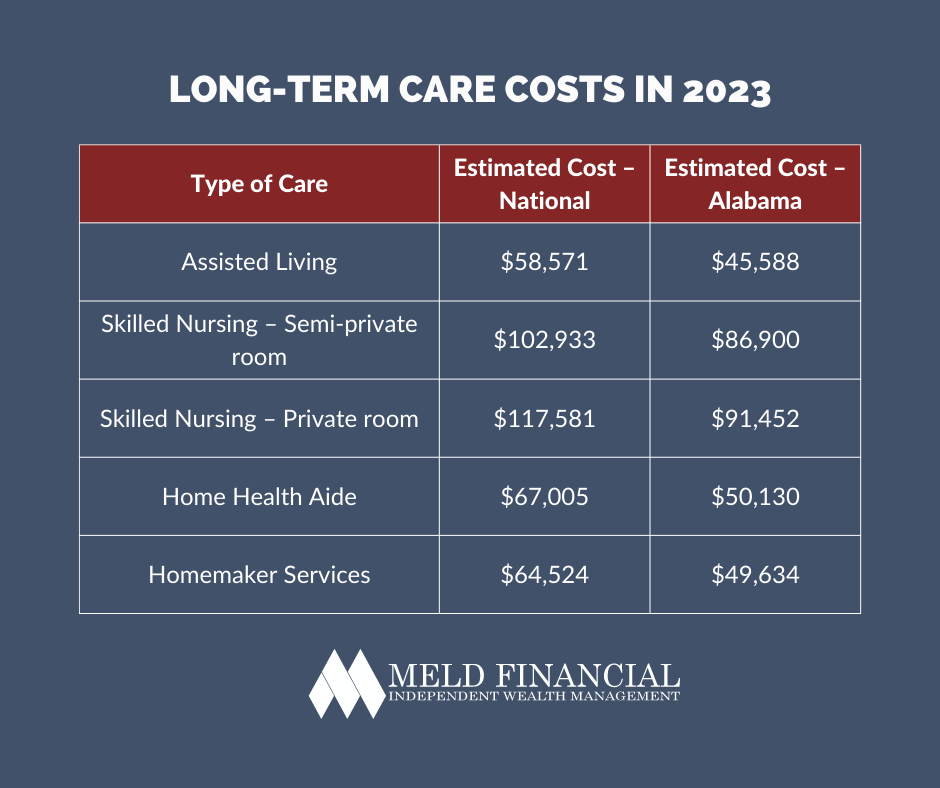
And it’s not just nursing homes. In some states, assisted living centers charge as much as $11,000 a month but offer no medical oversight and few staffing requirements. Hidden fees pile up fast. One recent analysis found that only a fraction of that monthly cost goes toward direct care. The rest? Rent, administration, and shareholder returns.
Meanwhile, the people doing the actual labor—home health aides, nursing assistants, elder companions—are paid poverty wages. Many are women of color. Most have no benefits. They are asked to do physically and emotionally demanding work with little support and no safety net.
As the human workforce collapses, the tech sector has stepped in, not with solutions but surveillance. From fall sensors and medication trackers to robotic “companions,” technology is being marketed as a replacement for human care. But machines can’t prevent loneliness. Algorithms don’t hold hands.
When care becomes a product, people become expenses. And in the for-profit elder economy, cutting expenses is the whole business model.
The Cost of Disposability
When elder care fails, it doesn’t just fray the edges; it tears through people’s lives. For millions of Americans, aging has become a slow-motion eviction from dignity.
Across the country, hospitals are discharging unhoused elders onto city streets, often without a plan, a phone call, or a follow-up. Nursing homes, overwhelmed and underfunded, quietly evict residents who run out of money or who require “too much” care. Some are dropped at shelters. Others die in transit.
For those who remain, the conditions can be just as dire. Dementia is increasingly criminalized; residents with confusion, aggression, or noncompliance are met not with compassion, but with law enforcement or chemical restraint. Some facilities medicate residents into silence just to maintain order.
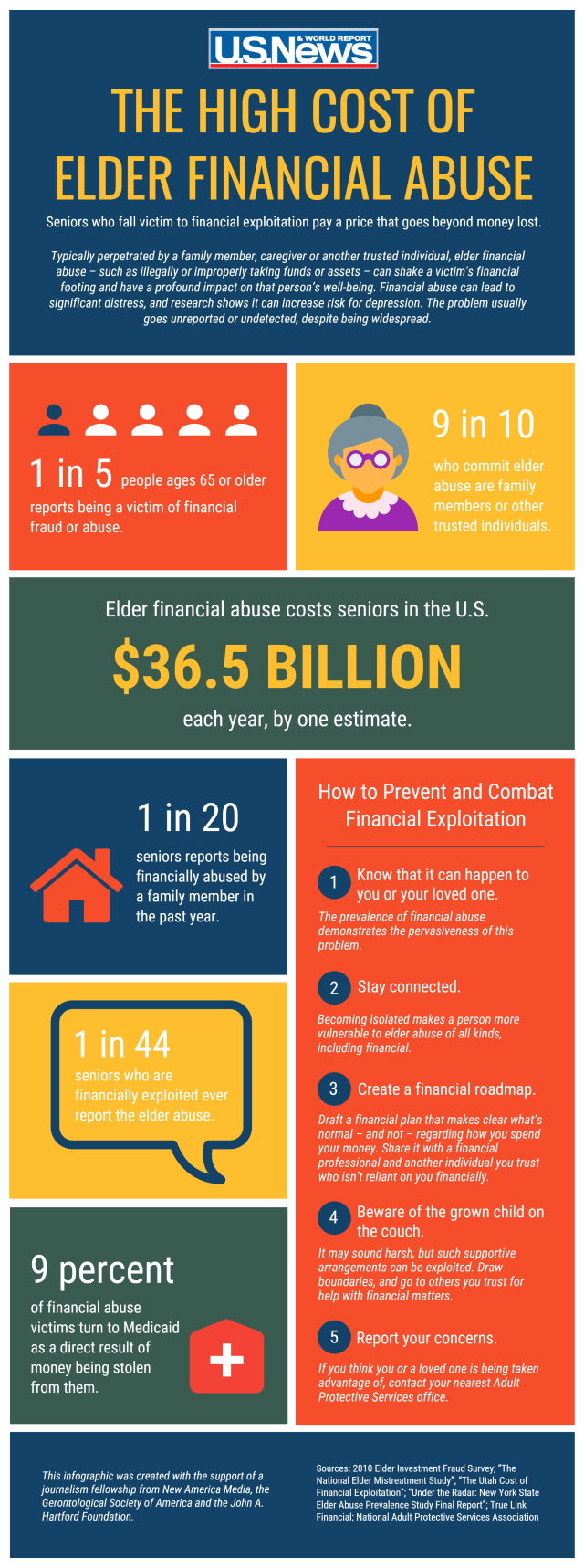
Behind closed doors, a quieter violence unfolds. In low-income housing and underfunded facilities, elders are routinely scammed, sometimes by family, sometimes by underpaid or overstretched caregivers. Medications go missing. Rent money disappears. Trust is exploited. And when residents report the abuse, they’re often ignored or disbelieved.
The suicide rate among Americans 75 and older has quietly surged in recent years, particularly among white men, who often face old age with fewer support systems and greater isolation. Elder mental health is underfunded, understudied, and stigmatized.
And we cannot ignore those aging inside cages. The number of people over 55 in U.S. prisons has quadrupled in the past 20 years. Many are incarcerated for decades-old offenses or parole violations. They live with untreated chronic illness, minimal mobility accommodations, and no meaningful access to end-of-life care.
The same is true in immigration detention, where older asylum seekers and long-term U.S. residents are denied basic healthcare and kept in conditions that violate human rights standards.
These aren’t accidents. They’re design features of a system that doesn’t see elders as people to protect, but as problems to disappear.
What Elder Liberation Looks Like
We don’t have to accept this. Aging doesn’t have to be a descent into isolation, indignity, or debt. We can build something better, but not by tweaking around the edges. We need a new foundation.
True elder liberation means ending the idea that care is a commodity and recognizing it as a collective responsibility. It means moving from warehousing to inclusion, from crisis response to long-term investment, from institutional control to interdependence and choice.
That starts with policy:
Fully fund home- and community-based services (HCBS) so elders can live in their own homes with the support they need.
Guarantee paid family caregiving leave and compensate informal caregivers for the labor they’re already doing.
Incorporate long-term care into Medicare for All: no more exclusions, no more spend-downs.
Ban for-profit elder facilities and reinvest in public or cooperative care models.
Raise wages and protections for home health and facility workers, with real training and union support.
Fund aging-in-place infrastructure: accessible housing, transportation, telehealth, and neighborhood-level services.
Ensure dignity in detention by expanding compassionate release and ending the incarceration of the elderly altogether.
Just as importantly, we must shift how we talk about aging. Not as a burden, not as a failure, but as part of the human story deserving of care, autonomy, and joy.
Elders are not disposable. They are our past, our present, and—if we’re lucky—our future.
We just hit 13,000 subscribers—thank you! We’re offering full access to The Coffman Chronicle at 50% off to celebrate.
Get exclusive analysis and fearless reporting you won’t find in corporate media.
Bibliography:
U.S. Census Bureau. "By 2030, All Baby Boomers Will Be Age 65 or Older." December 10, 2019.
Association of Private Equity Investment in US Nursing Homes With Cost and Quality of Care. JAMA Health Forum. November 19, 2021.
The Guardian. "In the US, Not Even $11,000 a Month Can Buy You Dignity at the End of Your Life." May 1, 2025.
MarketWatch. "$880 Billion in Medicaid Cuts Would Be 'Devastating' for Nursing Homes and Their Residents." May 3, 2025.
Lidsen Publishing Inc. "Using Elder Abuse Case Studies to Develop LGBTQ+ Cultural Competency." Geriatrics 8, no. 1 (2023): 266.
National Center on Elder Abuse. "NCEA Elder Abuse Annual Research Compilation, September 2022 – August 2023."
SeniorLiving.org. "How Much Does Assisted Living Cost in 2025?" Accessed May 8, 2025.
Stateline. "Medicaid Cuts Could Hurt Older Adults Who Rely on Home Care, Nursing Homes." March 28, 2025.
National Institute on Aging. "Spotting the Signs of Elder Abuse." Accessed May 8, 2025.
Population Reference Bureau. "Fact Sheet: Aging in the United States." January 9, 2023.
AARP. “Valuing the Invaluable: 2023 Update.” March 8, 2023.
Prison Policy Initiative. “The Aging Prison Population: Causes, Costs, and Consequences.” August 2, 2023.
Centers for Disease Control and Prevention. “Suicide Among Adults Aged 55 and Older, 2021.” November 2023.
Kaiser Family Foundation. “A Look at Waiting Lists for Medicaid Home- and Community-Based Services from 2016 to 2023.” November 2023.
Thank you so much for this well documented article. I have been seeing all of this unfolding, and as a senior citizen who is caring for another senior (victim of Covid) it is taking a toll. My disabilities are getting worse, and my insurance plus Medicare doesn't cover the needed operations I should have - despite the $185 premium I pay through Social Security. I don't know how much longer I can take care of him because I have trouble taking care of myself. I get paid $13.85 an hour for 3 hours per day/7 days a week. I am on call 24/7, and three hours is nowhere near enough time for all the things I have to do. Luckily we have a house, although not paid off yet, and my daughter and her sons live with us to help pick up the slack. How many don't have that much help? This is a system that really is against the aging, yet doesn't understand how much we have to give.
That’s incredibly well-defined. I would add one thing, from my perspective as a disabled 63 year old: in conversation with one of my kids last winter (she’s 27), I spoke about “filial piety,” in the context of “what’s going to happen to me when/if I can’t live alone?” She replied, “I know SOME cultures believe in that.” It was a bit scary to think that this ethical principle may no longer apply in the thinking of young Americans now.
I’ve actually moved abroad, where health care is not a privilege, but is an expectation built into the social system.