

They Cut the Lifeline First
Rural hospital decline is not just a healthcare story. It is what happens when Washington weakens one of the last institutions holding small communities together.


The Rural Rescue That Doesn’t Rescue
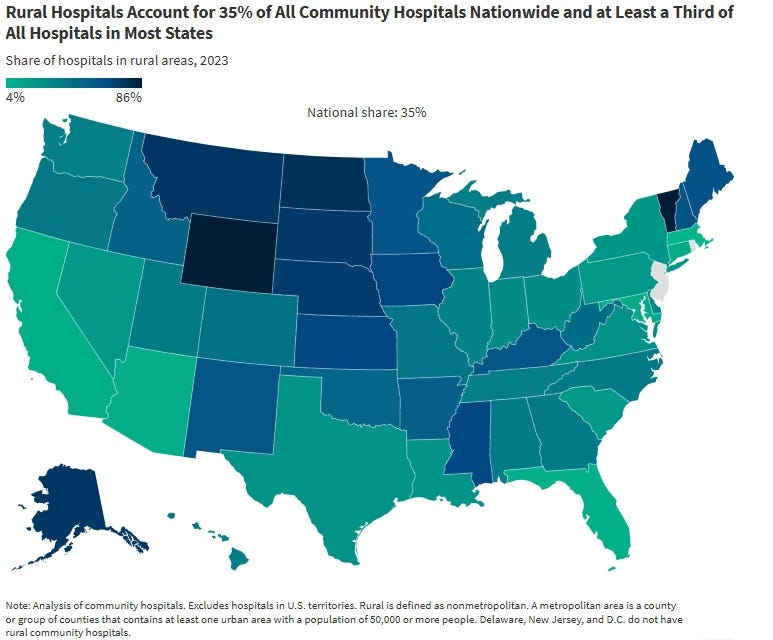
Rural hospitals were already hanging on by a thread before Washington decided to test how much more strain they could take. Reuters reported in March that the United States has about 2,000 rural hospitals, that more than 40% already operate at a loss, and that 417 are considered vulnerable to closure. That is not a system with room for ideological experiments. It is a system already living on narrow margins in places where the hospital is often the last line between a medical emergency and a long, dangerous drive.
Now the same political class that backed deep Medicaid cuts is trying to sell a temporary rural health fund as proof it came to the rescue. The numbers say otherwise. KFF (widely known as the Kaiser Family Foundation) estimates that federal Medicaid spending in rural areas will fall by about $137 billion over ten years, while the Rural Health Transformation Program provides $50 billion over five years. KFF also found that 64% of those Medicaid reductions arrive after 2030, which means the fund expires before much of the damage fully lands. That is not rescue. That is a partial patch with a better press release than balance sheet.
The system was fragile. Washington cut a major financing stream anyway. Then it offered a smaller, temporary program and asked rural America to call that protection. The argument is not complicated because the math is not complicated. The lifeline was cut first. The bandage came second.
This Community Is Powered by You
What started as a small circle has grown into something much bigger, and it’s all because of readers like you.
Every time you forward this email, post it on socials, or bring someone new into the fold, you’re helping build one of the most passionate, independent political communities out there.
Want to keep the momentum going?
Share this newsletter with someone who should be part of this conversation.
Thank you for being here. It means everything.
A Fragile System, Not a Sturdy One in Need of Reinvention
The weakness in rural healthcare did not begin with this law. It was already built into the economics of small-town medicine. Rural hospitals must maintain emergency departments, staff, beds, and basic services across large geographic areas while serving smaller, older, poorer, and sicker populations than many urban systems do. Reuters’ reporting shows why that matters: rural communities often start with fewer providers, worse health indicators, less access to specialists, and longer distances to advanced care. In that environment, even a modest policy shock hits harder.
KFF
That is why it is so misleading to talk about rural hospitals as if they were merely inefficient businesses overdue for “transformation.” They are not failing boutique retailers. They are often the only nearby place for emergency stabilization, basic inpatient care, and labor and delivery. When one of them weakens, the alternatives are not down the street. They are in the next county, or the next region, or an hour farther down the road. Reuters’ Kansas reporting makes the point vividly: once local capacity thins out, advanced cardiac cases, severe trauma, and complicated childbirth already mean transfer.
Washington didn’t inherit a sturdy system and tried to modernize it. The starting point is that policymakers were dealing with a fragile system that needed protection, stability, and sustained financing. Instead, they chose to weaken one of its biggest support beams.
Medicaid Is a Load-Bearing Beam
Medicaid is not some side issue in rural healthcare. It is one of the structural supports holding the system up. KFF estimates that about 66 million people live in rural areas, that Medicaid covers one in four adults there, nearly half of all births, and one-fifth of inpatient discharges. Those are not edge cases. They mean Medicaid is woven directly into whether rural hospitals can keep maternity care open, absorb emergency admissions, and get paid for serving lower-income populations with fewer private insurance options.
KFF
That is the part of Washington’s sales pitch that depends on people not fully understanding. In rural America, Medicaid is not just an insurance card in a patient’s wallet. It is part of the operating logic that keeps the local hospital functioning. These hospitals already have lower patient volumes and less of a revenue cushion than large urban systems. When policymakers cut Medicaid in that environment, they are not trimming around the edges. They are pressing on one of the beams that hold up the roof.
Once you see Medicaid that way, the “rural rescue” branding collapses. A government cannot significantly reduce one of the main streams of money that rural hospitals depend on, then point to a smaller, temporary fund and call the problem solved. The replacement is smaller, shorter, and less certain than the loss. That is not an ideological opinion. It is what the numbers show.
The Cut Came First, and the Patch Came Second
The sequence reveals the fund's real function. Washington did not look at a stable rural healthcare system, notice distress, and step in with relief. KFF reports that the rural fund was added late in the legislative process after concerns were raised about how the broader cuts would affect rural hospitals. In other words, the patch came only after the damage was politically obvious.
A real rescue would begin by protecting the financial base that hospitals already rely on. This approach did the opposite. The same law that created the five-year $50 billion fund also set in motion an estimated $137 billion decline in federal Medicaid spending in rural areas over ten years. That means the patch offsets only part of the loss, and only for a limited time.
The timing makes the mismatch even harder to defend. KFF found that most of the ten-year Medicaid reduction in rural areas arrives after 2030, while the rural fund ends in 2030. The program being promoted as relief is designed to expire before much of the fiscal pain is fully felt. That is not an accident in policy storytelling. It allows Washington to advertise immediate help now while leaving future communities to absorb the bigger losses later.
A Fund Built to Spread Credit, Not Solve the Problem
The fund's weakness is not just that it is too small. It was also built in a way that does not reliably send the most help to the places under the most strain. Half of the money is distributed equally among approved states, while the rest is allocated based on CMS measures of need and other administrative criteria. Further, the law does not require CMS to publish detailed distribution information.
Equal distribution may sound fair, but equal is not the same thing as targeted. AP reported that the administration’s formula also ties part of the funding to policy priorities it favors, and that some of the money can be recalculated annually and clawed back. KFF and AP both point to the same underlying problem: a state with fewer rural hospitals can still receive a base amount comparable to that of a state with far greater rural exposure, while some funding decisions are filtered through federal discretion rather than by direct emergency need.
In plain English, a fund that is already too small is also routed through layers of politics, scoring, and discretion that can pull it farther away from the hospitals hanging closest to the edge. That design is useful for Washington because it spreads credit broadly and creates a national talking point. It is less useful for a hospital that needs straightforward stabilization now, not a conditional invitation to compete for a partial lifeline.
What This Looks Like in Real Life
This is more than a budget fight. It is also a life-and-distance story. Reuters centered one part of its March reporting on Riley County, Kansas, where Ascension Via Christi is the county’s only emergency room. The same report described how advanced cardiac cases, severe trauma, and complicated labor-and-delivery cases already require transfer to larger hospitals. That is what fragility looks like before another major funding cut fully lands.
When a rural hospital weakens, the first losses are often not the building itself but the services inside it. Reuters reported that obstetrics is often among the first services cut when finances tighten. KFF says rural hospital closures and service reductions force patients to travel farther for care and can be especially dangerous for time-sensitive conditions such as heart attacks and childbirth. The result is not abstract. It is a woman in labor driving farther because the local maternity ward is gone. It is an ambulance spending more time on the road. It is an elderly patient delaying treatment because gas money, transportation, and time off work become one barrier too many. It is a rural equipment accident resulting in death rather than just injury.
The damage does not stop with patients. Rural hospitals are often among the largest employers and stabilizing institutions in small towns. Closures raise concerns not just about access to care but also about the broader local economy. Lose the hospital, and a community can lose payroll, healthcare workers, local confidence, and part of its ability to attract families or retire safely in place. That is how a healthcare story becomes a community-survival story.
Managed Decline Sold as Intervention
Rural America is praised constantly in campaign rhetoric as the backbone of the country, the part of America that politicians swear they will not forget. Yet when rhetoric meets arithmetic, the gap is hard to miss. Reuters reports that a system with hundreds of hospitals is already vulnerable to closure. KFF shows a ten-year rural Medicaid loss far larger than the five-year replacement fund. AP shows that even the replacement comes with strings, policy priorities, and uneven distribution.
That is why “rural rescue” deserves skepticism. A real rescue would have started by protecting the financing stream rural hospitals rely on most. Instead, Washington approved deep, long-run cuts, added a smaller, temporary patch when the political blowback became clear, and structured that patch to spread credit more reliably than to guarantee stabilization.
Conclusion
None of this means every rural hospital will close tomorrow. It means Washington chose to make an already fragile system easier to break, then tried to narrow the political fallout with a program that does not match the scale or duration of the loss. About 2,000 rural hospitals remain under strain. More than 40% already operate at a loss. Federal Medicaid spending in rural areas is projected to fall by about $137 billion over ten years, while the fund meant to soften the blow provides $50 billion over five years and expires before most of the damage fully arrives.
Those numbers do not describe a rescue. They describe a short-term patch laid over a larger long-term cut. And that is the point rural communities should not let Washington blur. The people who will pay first are the people with the fewest alternatives: the family facing a longer drive to the ER, the woman whose local maternity unit disappears, the town that loses one of its biggest employers, and the community told it was helped while one more essential institution slips closer to the edge. The lifeline was cut first. The bandage was never enough.
Support Independent Media
The Coffman Chronicle exists to follow power, expose the pattern, and tell the truth about who pays when Washington weakens essential institutions and calls the damage control a fix. If this kind of independent journalism matters to you, and you can afford to support it, please consider becoming a paid subscriber. Your support helps us keep doing the work corporate media too often skip, connecting policy decisions to the real people and communities forced to live with the consequences.
Sources:
“Trump Administration Announces Allocation of Rural Health Fund to States.” AP News, December 29, 2025.
“10 Things to Know About Rural Hospitals.” KFF, April 16, 2025.
“A Closer Look at the $50 Billion Rural Health Fund in the New Reconciliation Law.” KFF, August 4, 2025.
“Comparing States’ Rural Health Fund Allotments to Medicaid Spending Cuts Can Be Misleading.” KFF, February 6, 2026.
“How Might Federal Medicaid Cuts in the Enacted Reconciliation Package Affect Rural Areas?” KFF, July 24, 2025.
“The Fragile Economies at the Heart of Rural Hospitals.” Reuters, March 19, 2026.
As Dickens said in A Christmas Carol, “Let the poor die and decrease the surplus population.” This is what The Fapweasel (Trump) is doing, even if he never read the book or saw a production of the play or movie derived from it.
The MAGA Republicans are not friends of the farmers or their rural communities. Even before Trump they were fighting against Medi care and Medicade. They call these lifelines and Social Security, "entitlements". We need to get rid of that expression once and for all. The only entitled people according to Republicans (especially in the MAGA Trump regime) are billionaires. They cover themselves in white, elite entitlement. And it fits them, just like the white sheets they try to hide in their closets. It comes down to what do human beings deserve? And they don't deserve a bunch of politicians playing God with people's healthcare when they get their's bought and paid for by the American taxpayers (and not the billionaires).